
HEELS of different sizes are widely worn by women with the perception of increased attractiveness & for aesthetics purpose. But the regular use/ prolonged use of heels can alter the postural mechanics of body that may lead to increased pelvic tilt, pelvic rotation, uneven distribution of pressure on foot and knee.
High heels are those type of footwear where the heel area is higher than the forefoot area with a small toe section, curved plantar area, and a rigid heel cap.
How to Measure High Heels
| Heel category | Heel height (inches) | Heel height (meters) | Heel Height (cm) |
| Flats | Under 1 Inch | Under 0.025 m | 2.5cm or less |
| Low Heels | 1 inch – 2 inch | 0.025 m – 0.05 m | 2.5cm -5cm |
| Mid Heels | 2 inch – 3 inch | 0.05 m – 0.075 m | 5cm-7.5cm |
| High Heels | 3 inch – 4 inch | 0.075 m – 0.1 m | 7.5cm-10cm |
| Very High Heels | Over 4 inches | Over 0.1 m | Over 10cm |
The survey done by (Li et al., 2014) shows that between 39% and 69% of women wear high-heeled shoes on a daily basis for 1-8 hour per day. The effect of 3 cm, 6 cm, and 9 cm heel heights on adult women’s balance ability was studied and it was shown that balancing ability reduced as heel height increased.
Wearing high heels impairs the capacity to absorb and relay sensory information, as well as the afferent feedback system, which has an adverse impact on neuromuscular control and balance.
Effects of Walking with Heels
When the height of the shoe heel is high, the strides is shortened and the stance phase time is increased compared with the low heel. In another study, it was reported that high heels interfered with the ideal pattern of walking, reducing walking efficiency.
Effect of High Heels on Different Joints:
Ankle: They observed that enhanced plantar flexion in heel striking is required to overcome heel height while placing the foot on the ground. This is followed by an increase in the internal dorsiflexor moment during early stance. The ROM of the ankle joint declines in both the frontal and sagittal planes. In the sagittal plane, this is owing to the already plantarflexed foot and the activation of the tibialis anterior and triceps surea muscles. In the frontal plane during early stance, this is due to the diminished heel base, which prevents the foot from rotating without instability. This drop in ankle ROM is balanced by an increase in knee power generation.
Knee: The decreased ROM at the ankle joint (due to plantarflexion) is compensated at the knee joint by increasing knee flexion. The heel height reduces the ankle’s compliance. The foot is in a more plantarflexed posture & this lowers the moment lever arm of the ground response force, making the ankle joint less compliant, which is offset by higher compliance at the knee joint. During stance, a reduced and prolonged knee extensor moment was observed. Again, this can be explained by increased knee flexion in midstance. During the swing phase, less knee flexion occurs. This is compansated by elevating the hip of the swing leg.
Hip: An enhanced internal knee abduction moment occurs shortly after heel impact and before toe-off. The hip abduction moment rises throughout the stance phase, with the exception of heel striking. These two observations are seen due to the leg’s elongation as the heel height increases. During stance, hip flexion increases and is sustained in the late stance phase. This is connected with greater lumbar flexion (which leads to lordosis, as described below). The observed increase in hip ROM in the frontal plane is attributed to greater anterior pelvic roll.
Pelvis and Spine: During High Heel gait, the group of young women showed an increase in pelvic ROM in the sagittal plane compared to Low heel and barefoot conditions. It discovered that the lumbar flexion angle reduced by around 1 degree for every 1 cm rise in heel height. When compared to the barefoot condition, the Low heel and High heel conditions showed a substantial increase in erector spinae muscle activation at toe-off and during the initial contact period.
It was also shown that there is a substantial link between EMG data from the erector spinae muscles of the L4/L5 segment and vertical displacement of the Centre of Mass.
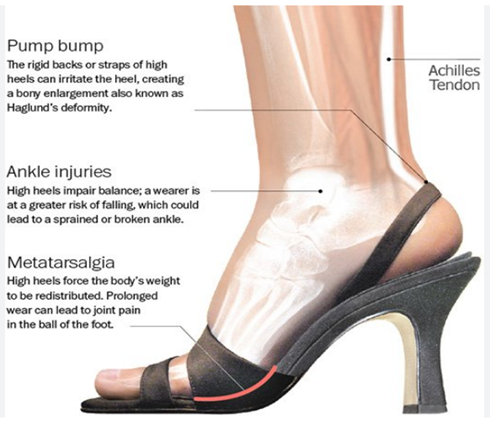
Following are the some conditions that you may face because of prolong high heels uses:
• Foot pain : (Hammertoe, Bunions, Morton’s Neuroma)
• Plantar Fasciitis
• Arthritis
• Balance issues
• Knee pain
• Hip pain
• Back pain
How to Wear High Heels
1. Always find the right shoe size, that makes you feels most comfortable and always fit
2. Don’t go for extreme height or the pencil heels instead of these try to wear a height of 0-4cm heels and should have wide base of support i.e platform heels.
3. Avoid pointed and less coverage heels.
4. Do not wear everyday, reserve them for special occasions.
5. If you walk to work, consider taking your heels with you and changing into them when you arrive.
6. Inserts can be used in your heel that help in better shock absorption & provide cushion to the feet. Eg. metatarsal pads, silicon pad for heel.